
Welcome to
Sky Women's Health
Menopause Transition & Sexual Health in Fort Worth, TX
OUR MISSION
Redefining Women’s Health Care
Sky Women's Health is a concierge gynecology practice in Fort Worth, created for women who are ready to feel seen, heard, and genuinely cared for. Founded by Dr. Carolyn Moyers—a board-certified OB-GYN, Menopause Society Certified Physician, and Fellow of the International Society for the Study of Women's Sexual Health—we offer unhurried, evidence-based care for perimenopause, menopause, and sexual health. Here, your concerns are taken seriously and your care is entirely your own.

Welcome to the neighborhood!
Imagine you get the kids to bed, your hair is up, glasses are on, and you slip out of the house for a sidewalk chat with your neighbor who happens to be an OBGYN. You laugh, you cry, you swap stories. She says vagina entirely too much! Best of all, there is no judgment between friends.
XO, Dr. Carolyn Moyers
Fort Worth Gynecologist
Membership
Escape the limitations of corporate medicine and insurance with Sky Women's Health. We invite you to experience a concierge women’s healthcare model that prioritizes you — a model centered on evidence-based, preventative holistic care delivered with the time and attention you deserve. Here, you're not just a patient; you're a priority. Join us in shaping a healthier future through our exclusive membership. Experience the Sky Women's Health difference, where personalized care is the norm.










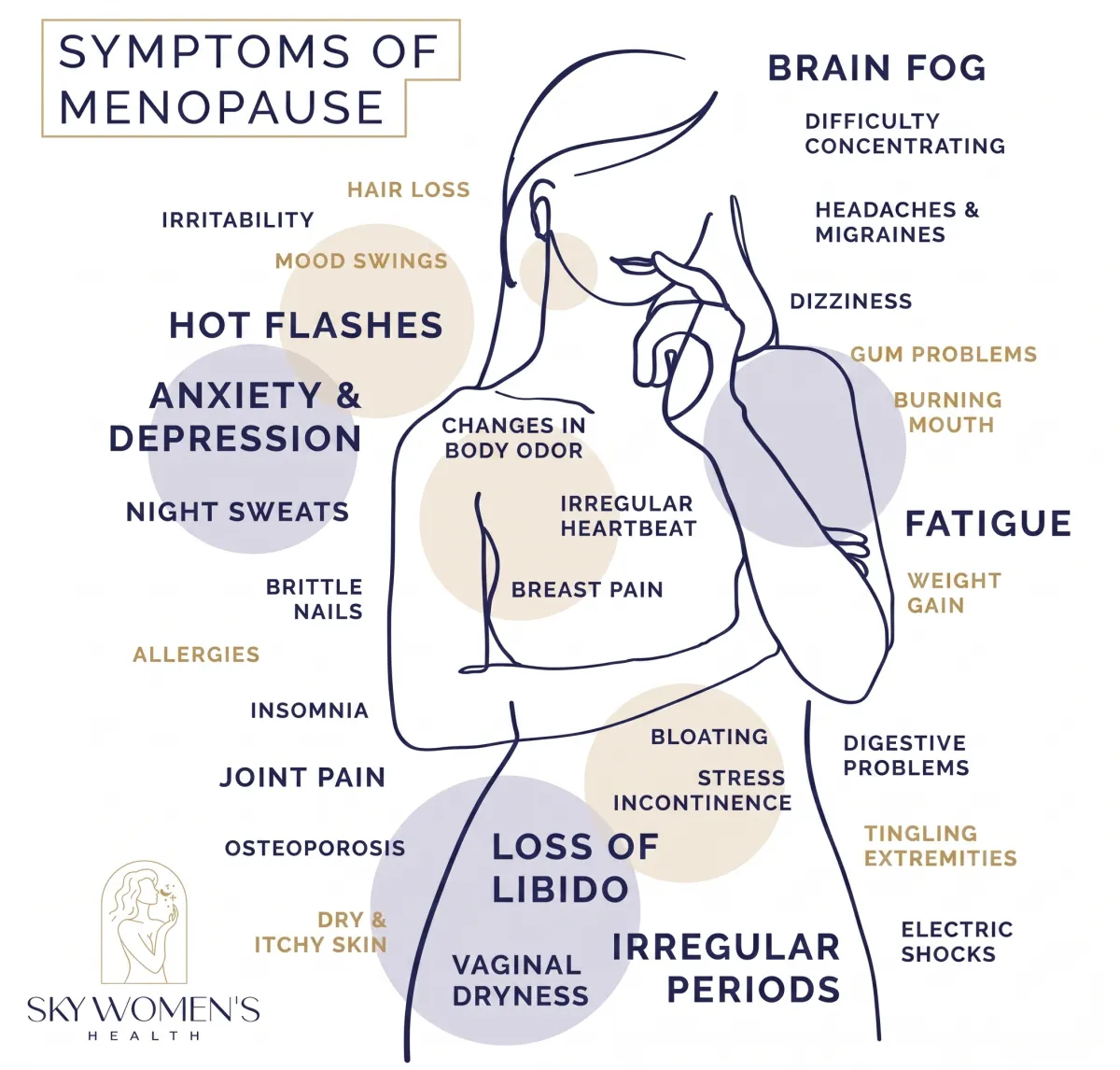
Don't Suffer Through Menopause Alone
Are you experiencing discomfort and frustration with midlife changes
"I finally found a place where I can talk openly about my symptoms
without feeling dismissed."
Jennifer T., CEO
Embrace Your Best Self Through Expert Menopause Care

Experience personalized treatment that helps you regain control, vitality, and joy during midlife.
• Personalized treatment plans tailored to address our unique symptoms and lifestyle needs.
• Convenient access to a certified menopause specialist dedicated to your well-being.
• Holistic care that not only alleviates symptoms but also empowers you to thrive in midlife.
• Ongoing support and follow-ups to adjust treatment and ensure your health journey stays on track.
FAQs:
How the Membership Works
What exactly is included in a Sky Women's Health membership?
This is not your typical doctor’s appointment. Your membership at Sky women’s health gets you the following:
Annual physical and up to eight (8) additional office visit appointments, including telemedicine.
✅ Priority scheduling
✅ Direct access to Dr. Moyers’ cell phone and email for after-hours communication
✅ Online access to personal health record
✅ Exclusive access to Sky Community Facebook group
✅ Access to join live podcast recordings, including live -Q&A sessions
✅ Nutritionist Program
✅ Complimentary consultation session with licensed professional counselor (LPC)
✅ Feel and look your best with quarterly InBody body composition scans and quarterly Osteopathic Manipulative Treatment (OMT)
✅ Coordination of specialist referrals
✅ Discounts on supplements (35%) and neurotoxin (10%)
✅ 20% Discount on surgical procedures
✅ ProNox for pain and anxiety relief for in office procedures at no additional cost
Each appointment is unhurried and uninterrupted. We're not watching a clock or rushing to the next room. You'll have real time to talk through what's happening, ask every question you came in with, and leave with a clear, personalized plan, not a pamphlet and a follow-up date six months out. We review your history before you walk in. We remember what you told us last time. We notice when something has changed.
My sex life has changed and I don't feel comfortable talking to my regular OB about it. Is this a safe place for that?
Completely and without reservation, yes.
Dr. Moyers is a Fellow of the International Society for the Study of Women's Sexual Health (ISSWSH) — a designation that signifies a commitment to excellence in the evidence-based practice of women's sexual medicine and health. The ISSWSH Fellow designation signifies training in the interdisciplinary, collaborative management of female sexual health — and it is a credential most OB/GYNs simply don't hold. It reflects not just interest in this field, but a demonstrated, ongoing commitment to advancing within it.
Pain with sex, decreased desire, difficulty with arousal, changes in sensation, relationship strain because of sexual health — these are all things Dr. Moyers addresses directly, clinically, and without judgment.
You will not be rushed past it. You will not be told it's normal or expected at your age. You will not have to find the courage to bring it up only to have it minimized. If it's affecting your quality of life and your relationships, it matters — and it belongs in the conversation.
How much does membership cost, and how do I pay?
Membership is available as an annual payment or monthly installments, whichever works best for you. For current pricing, contact our office directly.
We accept cash, credit card, FSA, and HSA funds. For healthcare expenses over $1,000, financing is available through CareCredit.
We know this is a real financial decision. What we hear most from patients is that membership didn't add to their expenses, it replaced years of fragmented spending on supplements, specialists, and treatments that never addressed the full picture. One practice. One plan. Care that actually works.
Does my insurance cover this?
Sky Women's Health is out-of-network with all insurance plans and is not enrolled in Medicare or Medicaid. Care is provided through membership, or fee-for-service.
That said, your insurance isn't completely out of the picture. Labs and Pap smears are submitted to your insurance for potential reimbursement, and FSA and HSA funds can be applied toward membership and services. CareCredit is available as an option to help finance expenses over $1000.
We operate this way by design. Insurance-based medicine dictates how much time a physician can spend with you, and for complex hormonal and sexual health concerns, that's rarely enough. Our model removes that ceiling. You get the time, the expertise, and a care plan built around your full picture, not a reimbursement code.
Can Sky Women's Health be my only doctor?
For gynecology, menopause, sexual health, and osteopathic care, yes, completely. You don't need another provider for those areas.
For women over 50 or those with complex medical histories, we recommend maintaining a relationship with a primary care physician. We coordinate closely with your existing providers - internists, cardiologists, therapists, etc., because integrated care produces better outcomes than specialists who never speak to each other.
What does a typical first visit look like?
If you've submitted medical records ahead of your visit, Dr. Moyers will have reviewed them before you arrive. Either way, your first visit isn't about starting from scratch — it's about going deeper.
You'll have a real conversation about your symptoms, history, goals, and everything connected to them. And because appointments are significantly longer than what you're used to, there's actually time to do it right.
Depending on your needs, your visit may also include a physical exam, an updated Pap smear, or a pelvic ultrasound (if clinically indicated). These exams are often able to be completed the same-day, without a separate appointment. Labs and imaging are frequently ordered so your plan of care can be tailored specifically to you.
You'll leave with clarity, finally. A real understanding of what's happening, why, and a personalized plan that includes both hormonal and non-hormonal options.
Are telehealth visits available, and do they count toward my 9 visits?
Yes. Telehealth is available to both membership and fee-for-service patients in Texas and West Virginia.
For follow-ups, medication management, and results reviews, a telehealth visit is just as effective as coming in, and often much easier to fit into a busy schedule. In-person visits remain necessary for procedures, physical exams, and certain treatments, but we're designed to flex around your life wherever possible.
What if I'm not sure what's wrong? I just know I don't feel like myself anymore.
That is exactly where we start.
You don't need to arrive with a diagnosis, a list of symptoms, or the right vocabulary. You don't need to have done your research or figured out what's wrong before you come in. What you need is a doctor who will actually listen, and then help you make sense of what you're experiencing.
"I don't feel like myself anymore" is not too vague. It's not in your head. And it is not something you have to accept. It's a starting point, and Dr. Moyers is very good at what comes next.
Is there a fee-for-service option if I'm not ready to commit to a membership?
Yes. If you'd like to experience the Sky Women's Health model before committing to a membership, pay-per-visit appointments are available at transparent cash pricing. You'll still get longer, unhurried appointments and Dr. Moyers' full attention, just without the continuity and discounts that come with membership.
That said, the membership exists because the best outcomes come from an ongoing relationship, not a single appointment. Hormones shift. Symptoms evolve. What works in year one may need to be adjusted in year two. The women who get the most out of this practice are the ones who show up consistently and let the care deepen over time. If you start fee-for-service and decide you want that kind of relationship, transitioning to membership is always an option.
What is the appointment cancellation policy and membership cancellation policy?
We require 72 hours' notice for cancellations or rescheduling. A credit card is required on file to secure your visit.
For members, your first two late cancellations are on us — no fee. After that, appointments canceled with less than 72 hours' notice, missed visits, or no-shows incur a $75 fee.
For fee-for-service patients, a $250 fee applies for missed or late-canceled new patient appointments, and $75 for return visits.
Membership is a one-year commitment. For details specific to your cancellation terms, please refer to your membership contract.
Does Sky Women's Health offer surgical procedures, and are those covered under membership?
Yes. Dr. Moyers performs minimally invasive gynecologic surgery with privileges at Baylor Scott & White, Baylor Surgicare, and Texas Health Resources Fort Worth.
Surgical procedures are priced separately from membership, and physician surgical fees are provided prior to scheduling so there are no surprises.
What membership ensures is that if you need surgery, you're not starting over with a stranger. Dr. Moyers already knows your history, your goals, and your concerns — and she's with you every step of the way, before and after.
What About My Labs and Pap Smear?
Your insurance isn't completely out of the picture.
Labs and Pap smears ordered through Sky Women's Health are processed through Path Advantage, an independent, in-office lab that is contracted with most major insurance plans.
Sky Women's Health is out-of-network with all insurance plans and is not enrolled in Medicare or Medicaid. Care is provided through membership or fee-for-service — and that's by design.
Insurance-based medicine dictates how much time a physician can spend with you. For complex hormonal and sexual health concerns, that's rarely enough. Our model removes that ceiling. You get the time, the expertise, and a care plan built around your full picture — not a reimbursement code. Path Advantage bills your insurance directly — it is a separate entity from Sky Women's Health — so your lab work and Pap results follow a familiar insurance pathway, even within a concierge model.
What to Expect Financially?
Surgical procedures are priced separately from membership. Physician surgical fees are provided in advance of scheduling so there are no surprises.
Facility fees, anesthesia, and pathology are billed through insurance directly by those respective providers — just as they would be with any in-network surgical experience. Dr. Moyers' team will walk you through what to expect before you ever confirm a date.
What Membership Means in a Surgical Context?
What membership ensures is that if you need surgery, you're not starting over with a stranger. Dr. Moyers already knows your history, your goals, and your concerns — and she's with you every step of the way, before and after.
For non-members who need surgical care, consultation is available. Contact the office to learn more.
How Can I Pay for Membership and Services?
Several options are available to make care accessible:
FSA and HSA funds can be applied toward membership and services
CareCredit is available to finance expenses over $1,000
Physician surgical fees are provided in advance of scheduling — no surprises
Patient Reviews
SERVICES WE OFFER
Conditions & Treatments

Sexual Health

Osteopathic Manipulative Treatment (OMT)

Menopause Care

Gynecology

Minimally Invasive Gynecologic Surgery
Telehealth

MonaLisa Touch®
Weight Loss
Navigating Midlife Changes Together
At Sky Women's Health, we understand the unique challenges of perimenopause and menopause, ensuring you feel heard and empowered every step of the way.
Top Doctor Recognition
Dr. Carolyn Moyers, recognized as one of Fort Worth Magazine's Top Doctors, offers compassionate, expert care tailored to women's health needs in midlife


Menopause Society Certified Provider
As a Certified Menopause Society
Provider and Fellow of the International Society for the Study of Women's Sexual Health, we provide specialized, knowledgeable care for your journey.

Thrive Through Menopause with
Customized Care
At Sky Women's Health, we understand the frustration of feeling dismissed by traditional medicine. Hot flashes, night sweats, and decreased sexual desire can disrupt your life, but you don't have to navigate these challenges alone. Our concierge membership offers you direct access to a board-certified, Menopause Society Certified Provider with specialized knowledge in your unique needs. Begin with an initial consultation to discuss your symptoms and medical history. Together, we'll craft a personalized treatment plan that may include hormone therapy and lifestyle modifications. Regular follow-ups ensure you receive the ongoing support you need to thrive in this important stage of life.
Now Accepting Telehealth
Appointments!
Schedule a virtual visit
Subscribe to our newsletter
Get weekly updates from Dr. Moyers
Fort Worth
1125 S Henderson St,
Fort Worth, TX 76104
Hours Of Operation:
Monday: 8:30 AM - 4:30 PM
Tuesday: 8:30 AM - 4:30 PM
Wednesday: 8:30 AM - 4:30 PM
Thursday: 8:30 AM - 4:30 PM